WHY TRUST US WITH YOUR BREAST RECONSTRUCTION?
WHY TRUST US WITH YOUR SURGERY?
Breast reconstructive surgery and other cosmetic breast surgery is regularly performed by Panthea Clinics’ specialist plastic surgeon Dr Farhadieh. Dr Farhadieh gained extensive subspecialty microsurgical experience at world leading institutes in London, England.
Breast cancer and reconstruction are a significant event in a woman’s life. It is vital that the patient and surgical team have a good relationship, coupled with realistic expectations. Perhaps the most important requirement is that the patient is provided with relevant information about the options available, so that she can make an informed decision about her treatment. Such information may be overwhelming, especially when you are coping with the sudden news of a disease such as breast cancer. Dr Farhadieh spends a significant amount of time during his consulting sessions listening to his patients, and explaining the surgical options, ensuring they have a clear understanding of the surgical pathway. Dr Farhadieh and his team endeavour to ensure that all patients feel supported during the entirety of their surgical journey.
If you have had a mastectomy and are thinking about getting breast microsurgery or reconstruction, get in touch with Panthea Clinics in either Canberra or Sydney. Our aim is to provide state of the art care for each and every patient, allowing you to feel great in your own skin once again.
WHAT WILL SURGERY ENTAIL?
BEFORE SURGERY
Smokers will be asked to cease smoking for at least 3-6 weeks prior to surgery and 3-6 weeks during the postoperative period.
You will be required to stop taking any medications, herbal remedies or supplements that may cause increased bleeding for at least 2 weeks prior to and 1 week following your surgery.
Depending on your age, medical and family history, you may be asked to have a screening mammogram prior to surgery
As there are many different options available for reconstruction, Dr Farhadieh will answer as many questions as you need to in order to understand the recommendations being made for you. There’s a lot to consider before undergoing breast reconstruction, and you should take the time to consider all options.
Dr Farhadieh will discuss all the potential risks and complications with you during your consultation. With Panthea Clinics, however, you can have complete peace of mind knowing that you’re being cared for by a team of dedicated specialists.
ON THE DAY OF YOUR SURGERY
Once your surgery day arrives, your incision lines will be marked while you’re awake and you will be able to ask any remaining questions as we go through our checklist with you. Breast reconstruction surgery is performed under general anaesthesia and patients will usually be discharged the day after surgery. Long-lasting local anaesthetic is injected into the surgical area, alleviating any immediate discomfort postoperatively. The incisions are closed using absorbable sutures before being sealed with dermal glue and covered with tape.
AFTER SURGERY
There may be some discoloration or mild swelling, however this will disappear quickly and will be completely resolved within 10-14 days. Throughout this healing time, straining, bending or lifting should be avoided and you should wear your supportive bra for at least 8 weeks. You will be able to go back to work within a few days of surgery and your breasts will find their final shape within 3 months.
FAQS:
WHAT IS THE DIFFERENCE BETWEEN IMMEDIATE VERSUS DELAYED BREAST RECONSTRUCTION?
There would logically appear to be a benefit in patients having breast reconstruction as a delayed second procedure sometime after their cancer surgery, in order to be more certain of the cancer clearance and to allow for adjuvant therapy. It would shorten their operative time, and allow for patients to adjust to life without a breast, thereby potentially deciding against reconstruction. Immediate reconstruction however allows for a one-stage procedure, and facilitates reconstruction when much of the breast skin envelope, and the inframammary fold (IMF), can be preserved.
Studies however have shown there to be no increased risk from an oncological standpoint. An increase in complications was identified, in particular wound infections. However, there was a definite patient preference for, and demonstrated psychological benefit from, immediate reconstruction. However immediate reconstruction carries with it service implications, those being greater interspecialty collaborative working.
WHAT SIZE AND TYPE OF IMPLANTS DOES DR FARHADIEH USE FOR ALLOPLASTIC RECONSTRUCTIONS?
Choice of implant size will vary from person to person and can depend on your body proportions and amount of breast tissue. It is important to be realistic with your desired breast size and consider Dr Farhadieh’s advice on what will work best for you and your body long term. The majority of the implants that Dr Farhadieh uses are smooth soft-gel silicone based implants.
WHAT ARE TISSUE EXPANDERS?
A breast tissue expander is an inflatable breast implant designed to stretch the skin and muscle and make room for a future, more permanent implant. They are commonly used in breast reconstructions that require two separate operations.
WHAT ARE THE RISKS ASSOCIATED?
There are inherent risks involved with all surgical procedures. While some risks may be minimal, others are potentially devastating for both patient and surgeon.
Surgical Complications:
- Haematoma (can lead to capsular contractures)
- Late seromas
- Device failure (recent generations of implants have proved to be more reliable)
- Early and severe capsular contracture
- Infections
- Wound healing problems
- Rotation/malposition of implants in alloplastic reconstructions
- Skin erosion
- Perforation followed by implant exposure
Aesthetic Outcome Complications:
- Wrinkling/rippling
- Asymmetries
- Scar formation
WHAT ARE THE RISKS ASSOCIATED WITH IMPLANT AND EXPANDER BASED RECONSTRUCTIONS?
These include infection, haematoma, seroma, wound dehiscence, skin flap necrosis, expander/implant deflation, capsular contracture, hypertrophic or keloid scarring, and venous thromboembolism disease. The strongest weighting, and therefore the risk factors that deserve the most caution, are smoking and obesity. Less weighted but nevertheless of significance is post-operative radiotherapy to both implants and to expanders. Diabetes, and pre-operative radiation are less significant, as are breast size, and hormonal or chemotherapy.
Gallery
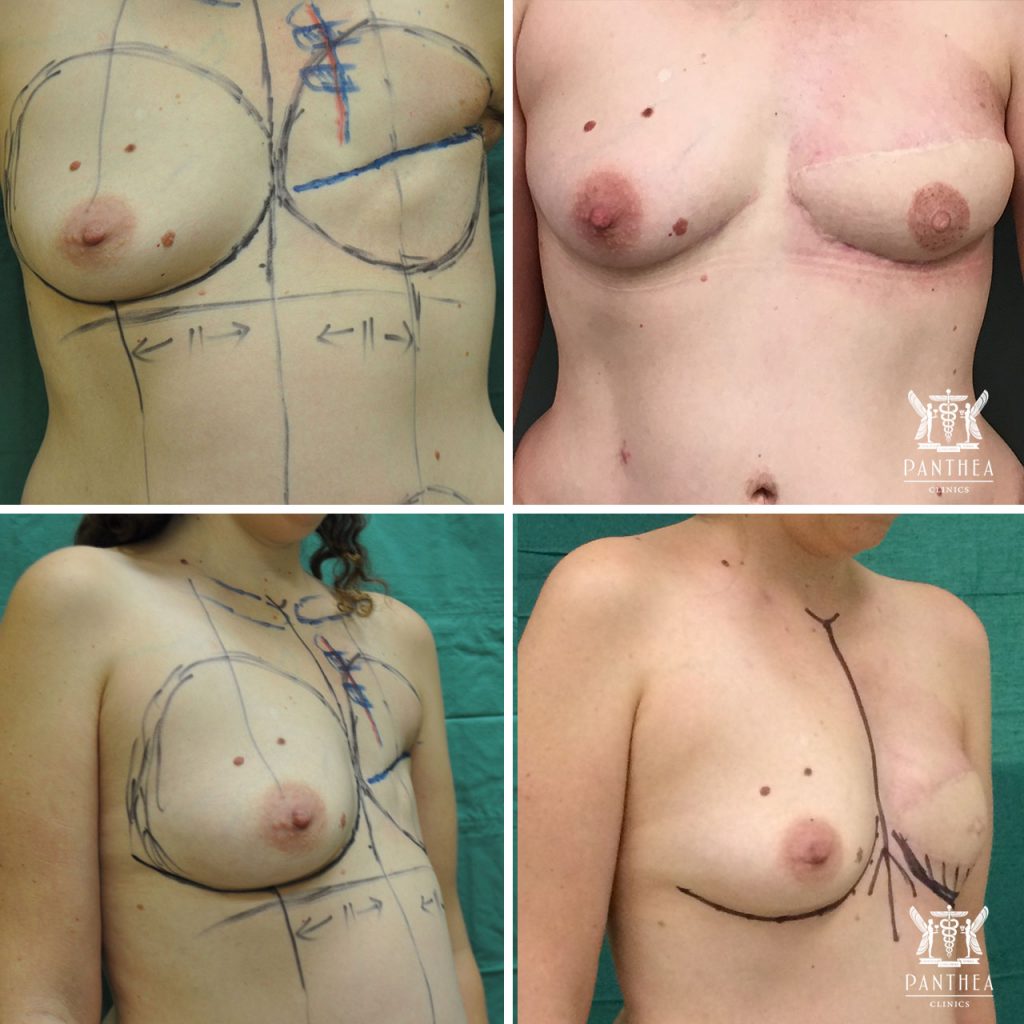
Delayed unilateral DIEP and nipple reconstruction.

Immediate DIEP microsurgical breast reconstruction of left breast with implant.
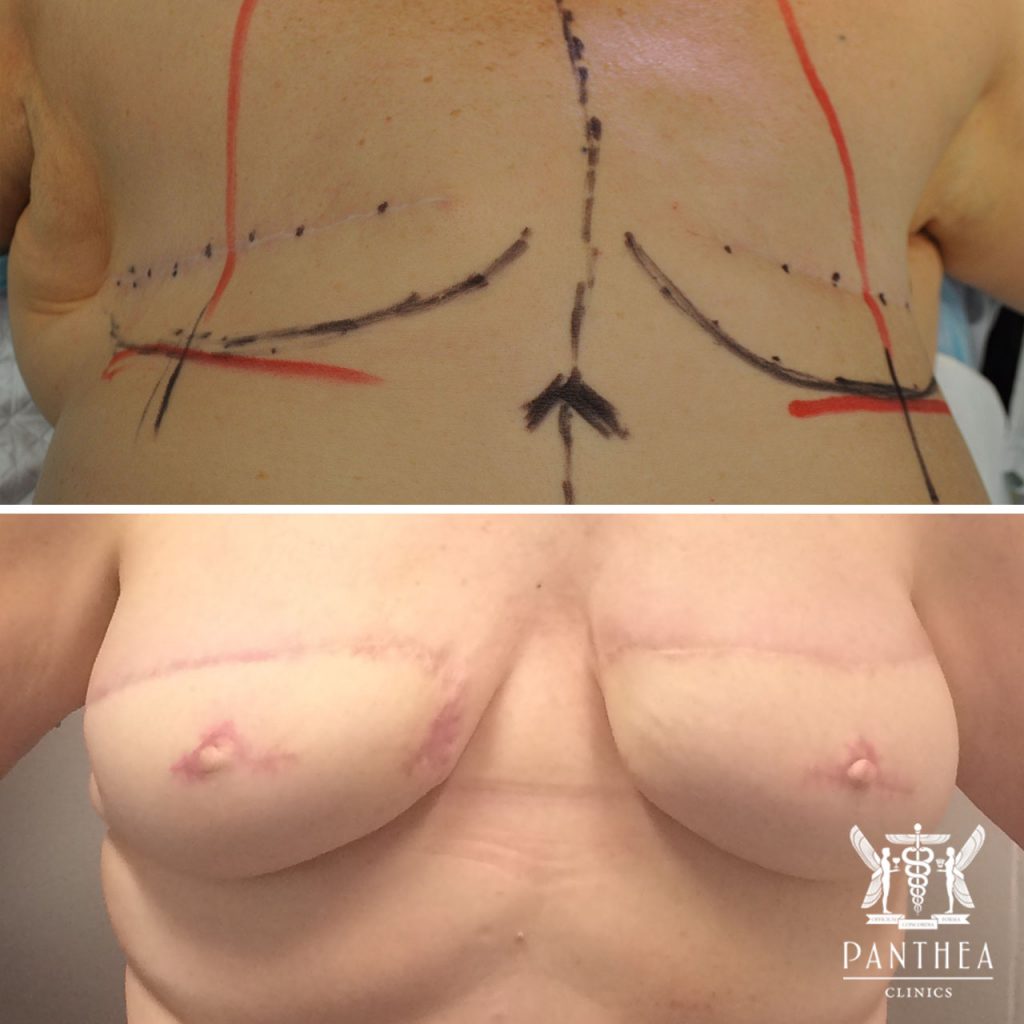
Delayed bilateral DIEP and nipple reconstruction.

A double DIEP, delayed DIEP on the left and immediate DIEP on the right.
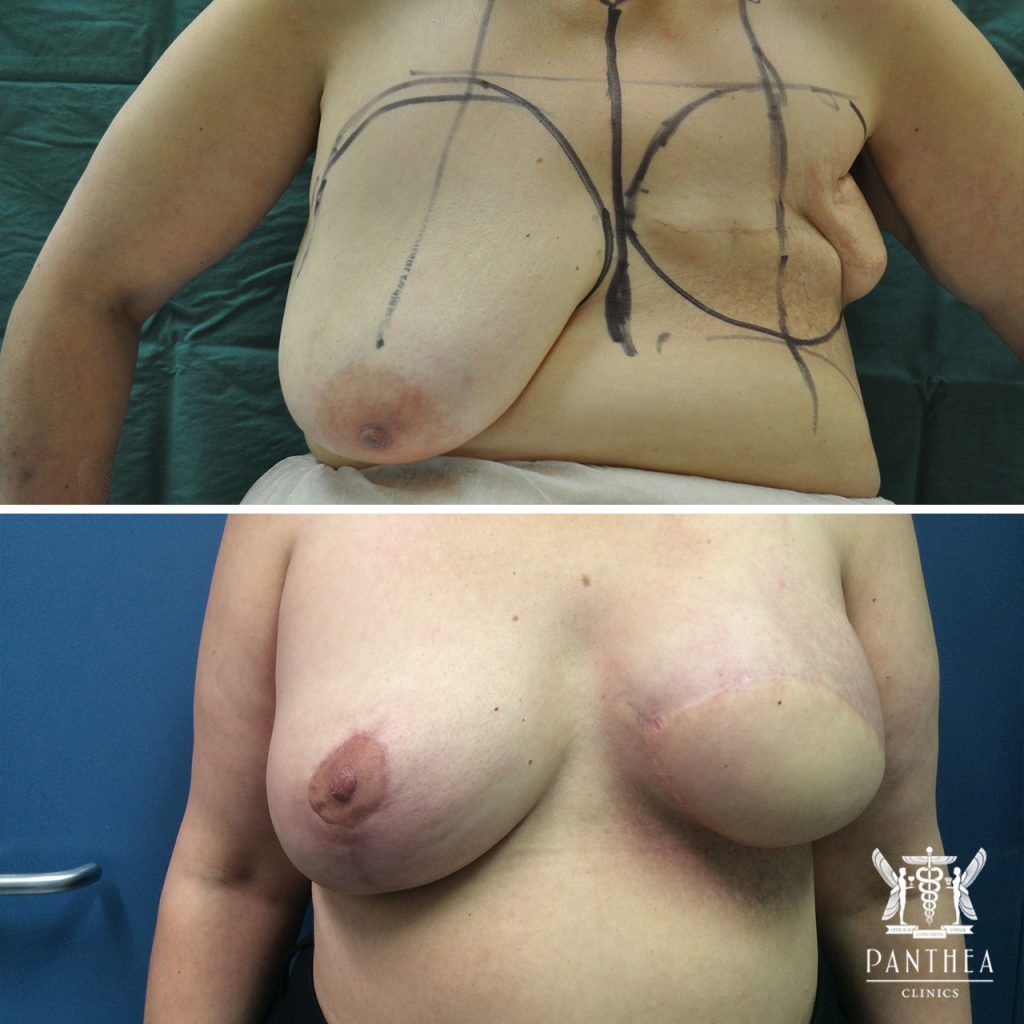
Right mastopexy and left Latissimus Dorsi flap and alloplastic (implant) reconstruction.

Immediate bilateral alloplastic (implant) reconstruction.